What is the Learning Unit about?
Electronic Health Records (EHRs) have become an integral part of modern healthcare systems. They structure clinical documentation, support communication between healthcare professionals, and increasingly incorporate advanced functionalities such as automated summaries, clinical decision support, and speech-to-text technologies. While these systems promise improvements in efficiency and continuity of care, they also introduce new challenges for healthcare professionals and students alike.
The LU106 learning unit was developed to help students critically engage with EHR systems, not simply as technical platforms, but as tools that actively shape clinical reasoning, communication, and patient care. The unit introduces learners to both the practical use of EHRs and the broader implications of digital documentation in healthcare settings. Students are encouraged to reflect on usability, workflow integration, patient access to records, data protection requirements, and the growing role of automation within clinical documentation systems.
A central feature of the learning unit is a virtual patient case built around Sibylle Jonas, a 66-year-old patient presenting with hyponatremia and syncope. While the presenting symptoms appear relatively straightforward at first, the underlying diagnosis – syndrome of inappropriate antidiuretic hormone secretion (SIADH) caused by small cell lung carcinoma – is intentionally concealed within the EHR documentation. Diagnostic clues are distributed across laboratory results, imaging findings, pathology reports, and clinical notes, requiring students to navigate the EHR carefully and synthesise information from multiple sources.
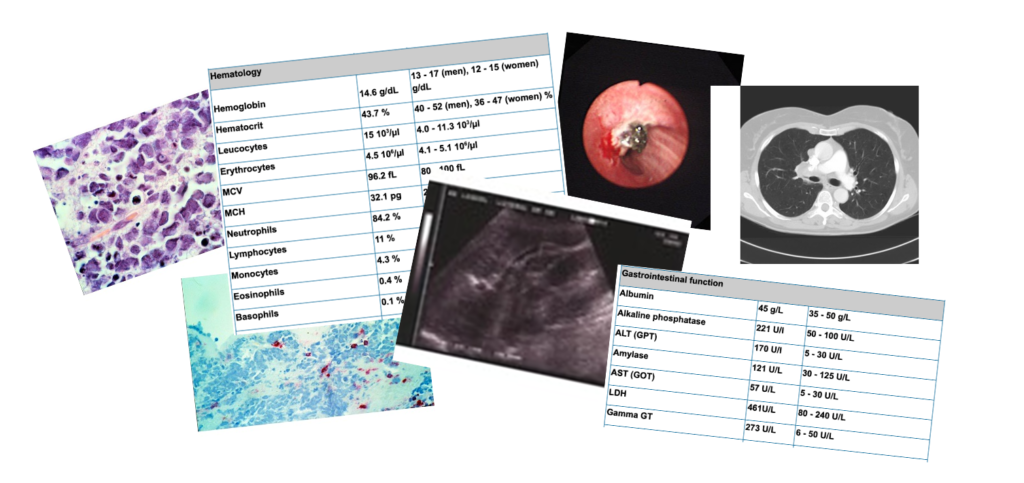
Rather than presenting EHRs as passive repositories of information, the learning unit highlights how the design and structure of digital records can influence clinical reasoning. Learners must determine which information is relevant, identify missing or fragmented documentation, and reflect on how interface design and workflow affect decision-making processes.
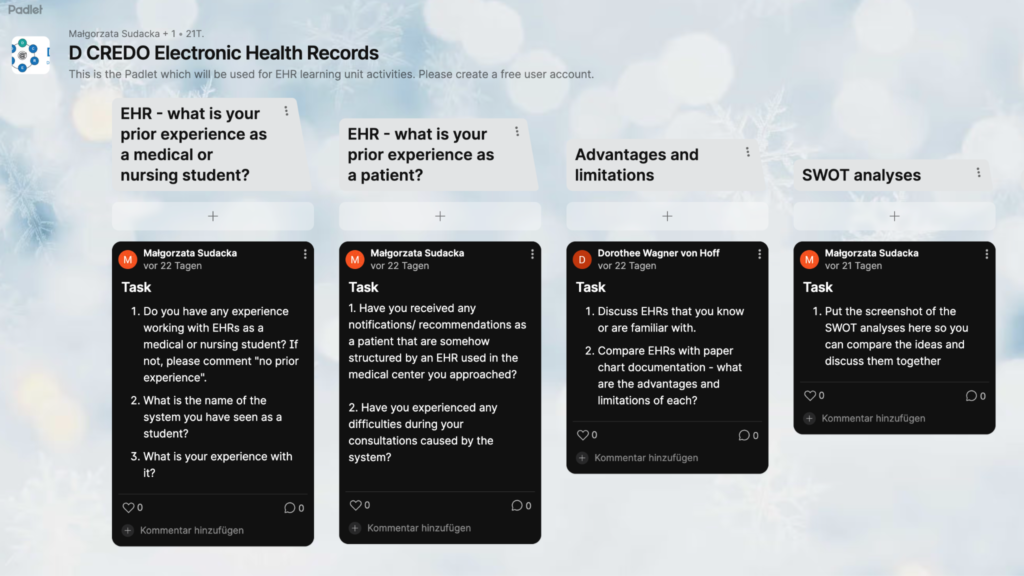
In addition to the virtual patient activity, students complete structured reflection tasks, including SWOT analyses and guided evaluations of EHR functionalities. These activities encourage learners to move beyond technical proficiency and critically assess the strengths, weaknesses, opportunities, and risks associated with digital health records in clinical practice.
Importantly, the unit also addresses the patient perspective. Students are reminded that patients increasingly have direct access to their own electronic records, which raises important questions about transparency, communication, and digital health literacy across different healthcare systems and countries.
How We Developed It
One of the biggest challenges during the development of LU106 was finding a way for students to experience EHR systems in a realistic and accessible manner. Many healthcare institutions use different EHR platforms, and not all educational settings have access to teaching systems or demo environments. From the beginning, we therefore aimed to create a learning unit that could function both in institutions with existing EHR infrastructures and in self-study settings.
Initially, the team explored several technical possibilities, including OpenEHR-based environments and existing demo systems. We also considered whether educators could rely on screenshots or static documentation alone. However, throughout the discussions it became increasingly clear that students benefit most when they can actively explore and interact with a realistic digital record system themselves.
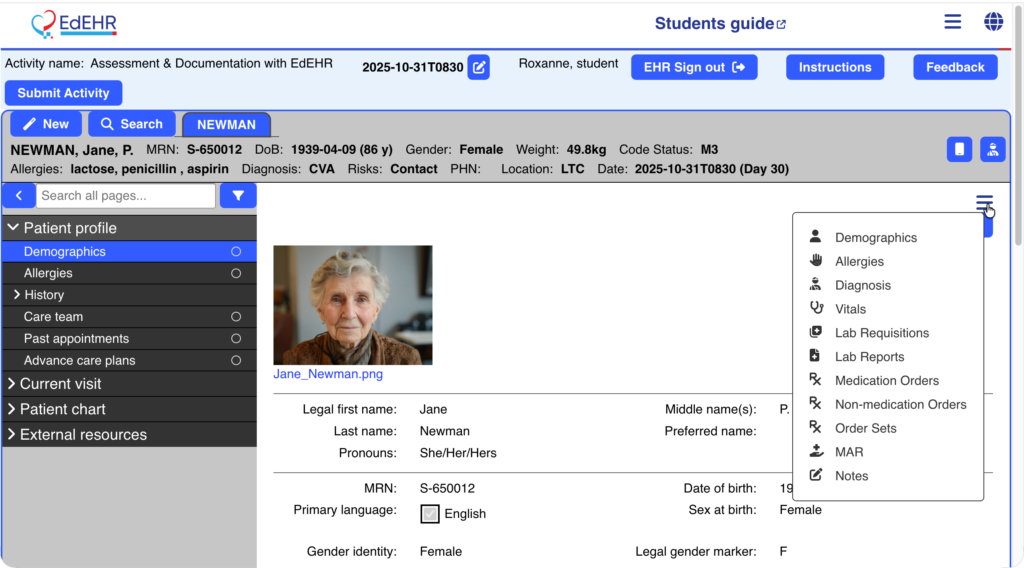
To support this goal, the team evaluated the use of an OpenEMR installation provided by the Jagiellonian University. This environment allowed developers to begin constructing the virtual patient case and testing how clinical information could be distributed realistically throughout the electronic record. At the same time, we recognised that not all institutions would be able to adopt the same platform. As a result, the learning materials were intentionally designed to remain transferable across different EHR systems. Laboratory findings, radiology reports, and other documentation elements are prepared in formats that educators could easily integrate into their own local teaching environments.
Accessibility and flexibility also shaped the pedagogical design of the unit. Introductory materials, asynchronous preparation phases, tutorial resources, and guided reflection exercises were developed to accommodate students with varying levels of prior EHR experience. This was particularly important because exposure to EHR systems differs significantly between healthcare programmes and institutions. While some students may already use EHRs during clinical placements, others may encounter them only late in their studies.
The reflection tasks became an especially important component of the learning unit. Since it was technically difficult to fully simulate advanced EHR functionalities such as speech-to-text documentation or automated clinical summaries, many of these topics were integrated into guided discussions and evaluation exercises instead. This allowed students to critically engage with current developments in digital healthcare even when direct technical implementation was not feasible.
What did we learn?
The development of LU106 reinforced how strongly digital systems shape clinical thinking and communication. EHRs are often perceived primarily as administrative tools, yet the process of building the virtual patient case demonstrated how profoundly the organisation and presentation of information can influence diagnostic reasoning. Even subtle design choices – such as where information is displayed, how laboratory trends are visualised, or how documentation is fragmented across different sections – can affect how learners interpret clinical situations.
Another important insight was the enormous variability in students’ prior experiences with EHR systems. Some learners are already comfortable navigating complex digital records, while others have had little or no exposure to clinical documentation software. This highlighted the importance of designing learning activities that remain accessible without oversimplifying the complexity of real-world digital healthcare environments.
Finally, the development process highlighted the growing importance of preparing students not only to use EHR systems, but also to critically evaluate them. As healthcare continues to integrate automation, AI-supported documentation tools, and patient-accessible records, future healthcare professionals will need to understand not only how these systems function, but also how they influence communication, clinical reasoning, equity, and patient trust.
Stay connected with D-CREDO and follow our journey on LinkedIn for more updates, insights, and stories.




